![]()
Kima Cargill is the author of The Psychology of Overeating: Food and the Culture of Consumerism (Bloomsbury Academic) and Associate Professor of Psychology at the University of Washington, Tacoma. She studies how the food and pharmaceutical industries use psychology to trick us into consuming more by distorting scientific information, sowing nutritional confusion, and convincing us that the solution to our problems is to consume more.

Contact: [email protected]
Sugar Highs and Lows: Is Sugar Really a Drug?
by Kima Cargill
Published April 2016
In the 1971 film Willy Wonka & the Chocolate Factory, little Charlie Bucket leaves behind his dismal, impoverished life by entering Willy Wonka’s magical factory. Sweetness is the balm that soothes Charlie’s pain and the viewer too is transported into a hypnotic world of confection in which the psychedelic imagery of flowing chocolate rivers and spinning candy pinwheels promises a regressive escape to pleasure, hedonism, and the intoxicating power of sugar. Although once thought of as an innocent, childlike high, sugar is now increasingly being called toxic and dangerous with calls by prominent researchers such as Kelly Brownell (2012) and Ashley Gearhardt (2009, 2011, 2013) for recognizing it as an addictive substance and regulating it as such. If successful, the outcome could be a great public health triumph.
Elsewhere I have aligned myself with these researchers and argued that the sugar industry is a menace to public health and should be subject to increased oversight and regulation (Cargill The Psychology of Overeating). At the same time, however, I have misgivings about the wisdom and validity of calling sugar addictive as a means to advance public health efforts. Although the sugar high has long been known to cause pleasure, reduce pain, and ameliorate dysphoria, the scientific evidence that sugar is addictive is mixed. Are those advocating for the recognition of sugar addiction rushing prematurely to a conclusion based on nascent neuroscience? If so, what does that mean for how we define, experience, and regulate pleasure and intoxication?
Because sugar is one of the few substances increasingly thought of as both a food and a drug, I argue here that it has become a flashpoint for two kinds of fear pandemics that have historically followed each—drug moral panics and nutritional scapegoatism. Sugar has taken on a symbolic valence in the current zeitgeist, mediating a see-saw of opposing forces governing the collective unconscious. On the one side is regression, pleasure, and intoxication—all historically viewed with moral suspicion and subject to suppression, control, and regulation. On the other side is scientific consensus, public health, and consumer protection. Underpinning (and perhaps fomenting) this tension is the impossibility of defining what makes something a drug.
By design I pose more questions than I answer. My aim is to provide a cultural and historical framework for understanding the current regulatory and scientific debate over sugar addiction. These questions are important because they frame not only how addiction is performed, but how science is performed. By that, I mean that both science and addiction are defined by empiricism, but at the same time they are shaped by tacit social construction. Posing questions about the tension between those two allows scholars across disciplines to better see the ways that scientific narrative is shaped by history and myth. Without this kind of hermeneutic lens, the reporting of scientific research in both academic journals and mainstream media takes on the appearance of unassailable, objective truth.
One recent such example of how scientific narrative was shaped by powerful cultural forces is the story of LSD (see for example Acid Test: LSD, Ecstasy, and the Power to Heal by Tom Shroder). In 1947, lysergic acid diethylamide was introduced commercially by Sandoz Laboratories as a legal, therapeutic psychiatric drug. Until the early 1960s, it was available to scientific and clinical investigators for medical research under the trade name Delysid. Then, after Harvard professor Timothy Leary began using and promoting recreational use of it, the cultural and political tides changed with the scientific community soon to follow. The pleasure provided by LSD, along with its association to the counterculture, undermined the idea that it was medicine. Even though no research ever came out suggesting that LSD didn’t have therapeutic applications, the scientific narrative changed, such that no university research on LSD was conducted for nearly fifty years (Slater). There is again, finally, a promising body of emerging research on the clinical use of psychedelics (Grob et al.), conducted by a group of self-proclaimed “serious and sober scientists” who aim to be “anti-Leary” (Slater). With LSD the cultural tides shaped scientific funding, research, and ultimately the narrative surrounding its clinical value and danger. I submit that similarly in the case of sugar, there is much going on in contemporary culture and politics that has pushed scientists toward identifying sugar as addictive, even though the evidence comes up short.
1. Sugar: Taste and Toxicity
For all of human history, people have enjoyed the taste of sweet. Humans and many other mammals are born with an innate liking for sweet which is stronger and more prevalent than the preference for any other taste. Since the 1960’s, scientists at the Monell Chemical Senses Center have been investigating the mechanisms and functions of taste and smell. Neuroscientists such as Linda Bartoshuk (1991) and Julie Mennella (1996, 1998) have found that the liking for sweet varies across cultures and is mediated by many factors. The pleasure, or hedonic reward, from sweetness is universal and is considered an evolutionary adaptation that encourages suckling because of the natural sugars in breast milk. The taste for sweet among humans is present not only at birth, but often in utero due to exposure to the maternal diet. Sweetness signals that food is safe and good to eat and discourages the consumption of spoiled or poisonous foods, which instead are often signaled by a foul odor or bitter taste. Not only does sweetness taste good, research has shown that it can reduce pain, alleviate depression and premenstrual symptoms, mediate stress, and activate the endogenous opioid system.
There is now no doubt that refined sugar consumed in large quantities can have toxic health effects and should be a concern for public health officials. Credit Suisse (2013) recently estimated that the consumption of sugar worldwide costs the global health care system $470 billion annually, representing over 10% of all health care costs and could rise to $700 billion by 2020. Sugar consumption is associated with numerous chronic diseases such as cardiovascular disease, obesity, high blood pressure and stroke. Many prominent researchers such as Robert Lustig (2012) and Susanne de la Monte (2005, 2012) are urging public health officials to redirect their focus from overweight and obesity to the staggering number of other diseases caused or influenced by sugar including cancer, Polycystic Ovarian Syndrome, and Alzheimer’s Disease, in addition to the cluster of disorders which constitute metabolic syndrome: Type II diabetes, hypertension, lipid problems, cardiovascular disease, and non-alcoholic fatty liver disease. Epidemiological studies demonstrate not only an association between obesity and cancer (World Cancer Research Fund/American Institute for Cancer Research), but increasingly there is evidence that it is not obesity, but independently the consumption of sugar which may contribute to the growth of certain types of cancer cells, particularly those with insulin. Epidemiologists such as Hu and Malik are now ringing alarm bells and saying that consumption of sugar is an independent primary risk factor that causes disease unrelated to excess calories, overweight, or obesity (Malik, Schulze and Hu; Malik et al. (Circulation); Malik et al. (Diabetes Care; Malik and Hu)).
It might seem evident that sugar or food can be addictive based on the rhetoric in popular culture. The 12-step program Overeaters Anonymous, for example, has long promoted the idea that food is addictive and has used the AA model of treatment for so-called food addicts. Yet, just as with AA, the language suggesting a neuroscientific basis for problem behavior was scientifically unfounded until recently when neuroscientists and addiction researchers such as Nicole Avena and Nora Volkow began to argue otherwise. Not only that, but also similar to AA, the prescribed treatment method for so-called food addiction has no empirical basis, and has, in fact, never been subject to any scientific evaluation.
Similar to other drugs of abuse, high-fat, high-sugar diets are associated with changes in the opiate and dopaminergic pathways of the brain in both rats and humans. There is also evidence that like other substance abusers, “food addicts” have similar personality characteristics and use food to regulate mood. Specifically, impulsivity is associated with the addictive consumption of food and individuals who report acting more rashly when experiencing urgent emotions endorse more symptoms of “addictive eating.” Other studies have shown that many self-identified food addicts use food to self-regulate in order to escape a negative mood state (Ifland et al.) and that high fat sweets in particular are frequently used to regulate emotions. Moreover, the combination of increased liking for carbohydrates in the context of decreased affect parallels how other drugs of abuse are craved and used as mood regulators (Corsica and Spring). For example, rats fed a diet of hyperpalatable foods show the behavioral signs of withdrawal, tolerance, and continued use despite negative consequences (Vanderschuren and Everitt) and individuals who display many symptoms of food addiction experience more food-related cravings and demonstrate more intense neural activation when consuming highly palatable foods (Gearhardt, Corbin, and Brownell; Gearhardt et al.). In other words, scientists have shown that 1) sugar and hyperpalatable food affect the brain in similar ways as some drugs of addiction, and 2) that some humans and rats use sugar in ways that are similar to drug use.
Other studies by addiction and obesity researchers like Mark Gold and Kenneth Blum have shown an inverse relationship between BMI and illicit drug use, a lower risk for substance use disorders in obese individuals, and lower rates of nicotine use and marijuana abuse, suggesting that overeating attenuates the use of other drugs possibly because the food itself functions as a drug. Not surprisingly then, in what is increasingly referred to as addiction transfer, food can become the new drug of choice as a result of alcohol or drug abstinence, often leading to weight gain among recovering addicts (Gold, Jacobs and Frost-Pineda).
In addition to the neurological reward provided by sugar, many researchers are now arguing that the production of refined sugar is more similar to the production and refinement of drugs of abuse than to the natural energy resources we historically consumed, like fruits, vegetables, nuts and meats (Gearhardt et al.). Such chemical alterations are the hallmark of drug production they argue, and provide elevated potency and rapid absorption into the bloodstream. The natural coca leaf for example, is only a mild stimulant (Hanna and Hornick), but when highly refined into cocaine or crack, it delivers an exponentially stronger hedonic reward and is far more addictive (Verebey and Gold).
In spite of this emerging body of research, there remains much disagreement over the concept of food addiction in the scientific community. One group of researchers rejects the notion of addictive food or eating, noting that there is little to no evidence for tolerance or withdrawal. Food cravings are not indicative of addiction they say, because the brain requires a constant supply of glucose for normal functioning and such cravings are fundamentally different than the cravings for drugs like cocaine or heroin which have no essential function for survival (Blundell, Coe, and Hooper 219). As for sugar’s effect on the dopaminageric reward system, they argue that there are a great many stimuli that can cause activation of dopaminergic areas, such as exercising, listening to music, or viewing art; yet those activities are not considered addictive. Finally, they note that the neurobiological research on sugar’s effect on the brain is limited to rats and similar effects have yet to be proven in humans.
A second faction of opposing researchers led by Hebebrand and Ziauddeen, acknowledge addictive-like eating behavior, but call “food addiction” a superficially attractive explanation which lacks systematic evidence (Ziauddeen (2012) 296). They argue that “food addiction” is a misnomer because “foods are nutritionally complex and there is hardly any evidence to suggest that under normal physiological circumstances humans crave specific foods in order to ingest a specific substance (299), and instead suggest that, if anything, the term “eating addiction” (295) would be more accurate because it focuses on the behavior, rather than the ingestion of a single addictive substance. This view places eating addiction in the realm of behavioral addictions like gambling, which are also recognized as addictive disorders, but are different than substance use disorders in that the focus is on excessive, repetitive behaviors rather than pharmacological mechanisms of drug use.
Psychobiologist John Blundell (2014) cautioned against the broadening of the addiction model, noting that already in popular culture, the term addiction is now used colloquially to describe anything done to excess, like shopping, having sex, and playing video games. Inappropriately broadening the addiction model risks losing the explanatory power and the neurobiological grounding of the model (Ziauddeen and Fletcher). As Blundell puts it “Overconsumption of food represents overconsumption in our culture. So we don’t need a neurochemical theory to explain it” (220). This is not to say that overeating delicious foods is not motivated by the brain’s reward system, nor that there are not real emotional problems associated with overeating. But there is a broader American, and, increasingly, global phenomenon of voracious overconsumption of all things: food, pills, electronics, gasoline, and luxury goods that have created the cultural and economic conditions for overconsumption on an individual level.
2. Moral Panics and Scapegoats
Of course, the determination of whether something is addictive or a drug requires the impossible task of defining those terms. Should it feel good? Make you want more? Get you high? Cause withdrawal? It depends on whom you ask. In keeping with the current dominant neurological model of mind, the medical community defines addiction as a chronic brain disease involving reward, motivation, memory and related circuitry (Smith). Yet other scholars have challenged this “neurocentricity” and suggested that there has been a careless rush toward conclusions and premature applications of nascent neuroscientific research (Satel and Lilienfeld).
An even broader critical approach suggested by Derrida is that there simply is no objective, scientific, or physical definition of a drug—that instead, “it is a non-scientific concept that is instituted on the basis of moral and political evaluations” (229). Accordingly, if we accept addiction as social construction, then we might also consider the extent to which labeling substances as a drug causes individuals to “become” users (234), as argued by sociologist Howard Becker in his seminal paper “Becoming a Marihuana User.” To put it in more psychological terms, the act of addiction, when thought of this way, is simply a sanctioned means of expressing distress, such that the move toward calling sugar a drug places it in the repertoire of addictive substances people have to choose from when performing addiction. However, given that a large portion of the aforementioned research on sugar addiction is on self-identified addicts, it raises the question of whether these studies are empirically investigating a group of people with a shared neurobiological problem or pathologizing a group of people with nothing more than a shared social identity.
Medical anthropologists such as Richard Castillo (1997) call the ways in which we learn to perform psychological distress is with the concepts of “culture bound syndromes” (37) or “idioms of distress” (29). Such illness metaphors are defined by a set of recognized behaviors, symptoms, and language which communicate sickness. All cultures have such tacit symptom repertoires offered to its people as a means of expressing distress—an internalized menu from which we unconsciously choose symptom sets as ways to express the difficulties of living. From my view, thinking about illnesses as culture-bound does not rule out possible biological or neurological causes, it simply redistributes the locus of origin onto the culture, and not just onto or within the individual. In other words, a disorder might well originate in neurochemical or neuroanatomical pathology, but be activated or exacerbated by cultural pathology—a view also held by the American Psychiatric Association (2013).
Even if there are multiple valid addiction concepts, it still seems that the semantic ambiguity leads to a conflation between the moral and the scientific. For even the scientists promoting the sugar addiction concept have attached moral attributes to sugar itself, suggesting that they too are responding to the cultural and historical associations to sugar. For example, in describing John Yudkin’s 1972 seminal anti-sugar book Pure, White, and Deadly, contemporary endocrinologist Robert Lustig calls it “prophetic” and refers to himself as a “Yudkin accolyte” (Smith)—terms with clear religious, even cult-like overtones: “Everything this man said in 1972 was the God's honest truth and if you want to read a true prophecy you find this book . . . I’m telling you every single thing this guy said has come to pass. I'm in awe” (Smith). In Lustig’s viral lecture Sugar: The Bitter Truth, he refers to sugar as evil, meanwhile others, like science writer Mark Schatzker, have taken to calling it “White Death” (8).
Moral panic over sugar is actually nothing new. Sugar has been accused of causing mental excitement, sexual depravity, and hyperactivity, with many people still continuing to mistake sugar consumption as a cause of AD/HD. The famous “Twinkie Defense” used by Dan White who killed San Francisco mayor Harvey Milk argued that sugar caused homicidal behavior (Gray). Folklore and fairy tales tell us that witches use sweets to lure innocent children into their lairs. And of course pedophiles use candy to lure children into their windowless vans. I submit that sugar has become a convergence point for two distinct types of collective fear: drug moral panic and nutritional scapegoatism.

There is of course a lengthy history of fears about drugs, with various inebriants and intoxicants taking center stage at different times. Scientific consensus, public opinion, and regulation of such substances have changed over time and across cultures, but contemporary Western history has largely defined such substances by their intoxicating properties, bolstered by widespread suspicion of intoxicated states (at least until the pharmaceutical industry co-opted intoxication as a form of treatment and legitimized drug taking via the ritual of doctor and pharmacy, as we can see most clearly in the recent decades of stimulant drugs such as Adderall for AD/HD).
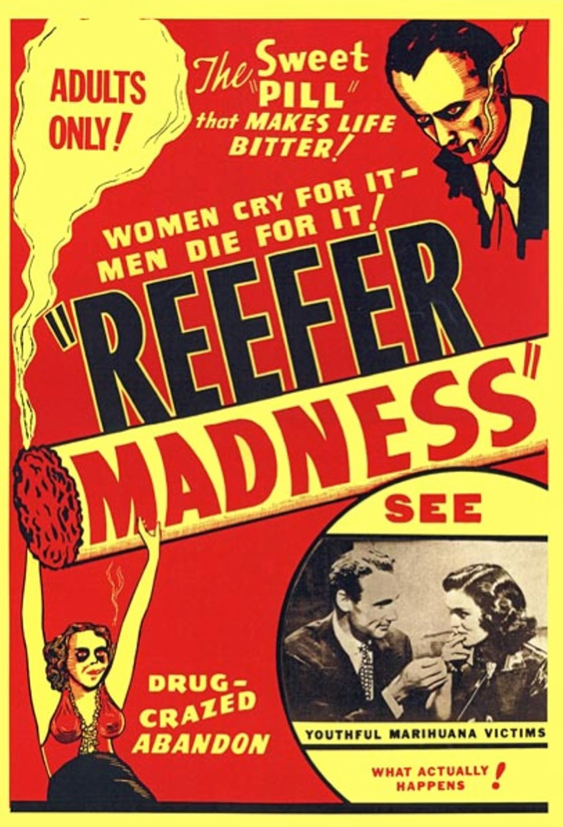
The public perception of sugar is now following the same path of moral panic seen with many other drugs, ranging from absinthe to marijuana. Note that the threat in a moral panic may be genuine and even harmful, but the alarm raised falls short of the threat and the imagined harm or cost to society balloons beyond what the evidence indicates (Goode and Ben-Yehuda). We might think of the pleasure and intoxication provided by drugs as a threat to the Victorian/Puritanical self in which sexual, aggressive, and otherwise base animal instincts could be unleashed. Freud and Darwin both challenged the widely held belief of the controlled, superior status of humans over other animals, and instead advanced a primivitized human self, with Freud in particular confronting Victorian culture with his “cauldron full of seething excitations” that is the id (537). Intoxication is, of course, a regressed or disinhibited state in which these sordid forces of the unconscious might bubble over that cauldron, representing dangerous threats to the ego.
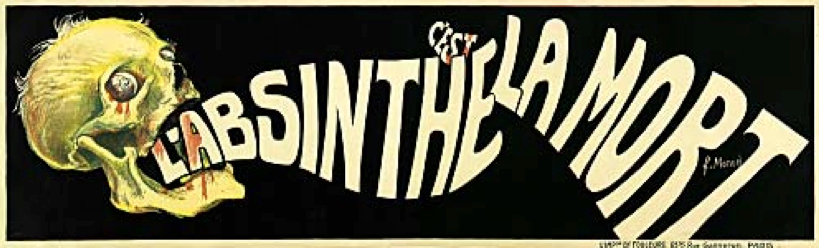
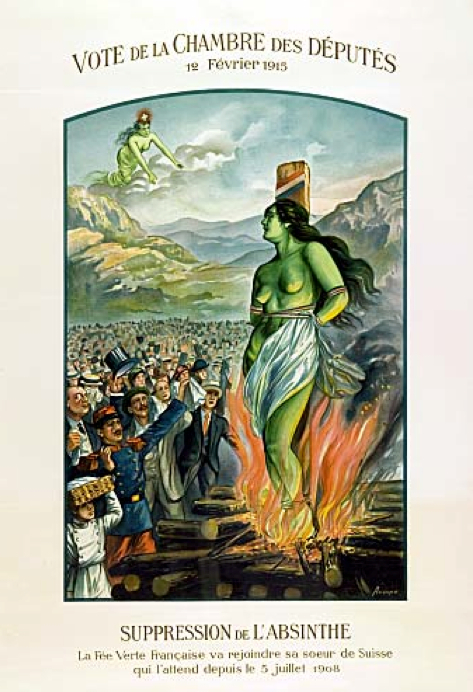
The historic imagery and rhetoric surrounding substances like marijuana and absinthe show that many drugs, and in particular their intoxicating properties, were viewed as dangerous, uncontained, potentially psychotic forces. Although partially true in some cases, these substances became scapegoats and symbolic repositories of forbidden impulses during the temperance movements throughout Europe and the United States. As I have argued elsewhere (Cargill “The Myth of the Green Fairy”), absinthe, for example, was reported to cause euphoria, mania, seizures, violence, hallucinations, blindness, even enlightenment, and rose to mythical proportions in the popular imagination. Recent laboratory studies however, have repeatedly shown that absinthe does not possess hallucinogenic nor aphrodisiac properties, as had long been thought. Yet until quite recently, absinthe was portrayed as a mysterious and dangerous substance, capable of inducing psychosis and aggression. I have previously suggested that absinthe became a repository for projected cultural fears about sexuality, madness, and aggression, as can be seen in early imagery surrounding absinthe. In France and Switzerland in particular, absinthe served as the battleground for the temperance movement and posters and postcards from that era personify absinthe alternatively as a sexualized temptress or a menacing grim reaper. Sugar too has now come to represent sex and death or Eros and Thanatos, as we see in the imagery and associations of sugar to Valentine’s Day, Halloween, and Day of the Dead.

Perhaps it is simply human nature to seek a means to personify and externalize such regressed, dangerous, and sordid forces? Of course these forces actually reside within—madness, sexual depravity, and aggression. Externalizing them is a means of reducing the anxiety they produce—the anxiety surrounding homicidal, adulterous, and psychotic impulses. In “The need to have enemies and allies” psychoanalyst Vamik Volkan calls this phenomenon “suitable targets of externalization” (226), that is, the seeking of comfortable and appropriate symbols serve as repositories for our fears. Historically such suitable targets of externalization were witches, the devil, or evil spirits, but in Western and increasingly secular societies such primitive targets hold less appeal and explanatory value. Immigrants, drugs, Y2K, vaccines, and food make far better targets in a culture which places a premium on science and technology. Explanatory models—suitable targets of externalization—that are premised on science and technology hold the most appeal and feel the most valid. This is perhaps why the neuroscience of “sugar addiction” is extremely compelling and has gained such momentum.
Yet, for many drugs the pendulum almost invariably swings in the other direction in the public imagination. For example, the acceptance and legalization of absinthe and marijuana is on the rise, as well as increasing research into the therapeutic effects of drugs like ecstasy, ketamine, and LSD (Preskorn). In some ways sugar is the new weed, which suggests that cultural fears about fatness and disease have eclipsed the moral concerns over regression and pleasure that drove previous drug moral panics.
Just like drug moral panics, there is also a lengthy history of seeking a single ingredient as the culprit for our ills: MSG, dietary fat, cholesterol, and gluten have all had their moments. Ultimately forms of magical thinking, there is tremendous psychological allure for these explanations. Not only do people seem to have an innate desire for simple, albeit implausible, explanations for complex phenomena (e.g., God made Eve from Adam’s rib), but also people have a powerful attraction to magic bullets—simple solutions that cure all ills.
Importantly, scientists themselves are not immune to the effects of such magical thinking. Many scholars and journalists have chronicled how even well-credentialed nutrition researchers have a history of getting it wrong and jumping on the bandwagon of nutritional scapegoatism (Taubes; Levinovitz). To be fair, good science is a lengthy process of mistakes, replication, and validation that often gets it wrong for many years before consensus is formed. It is this very messiness and uncertainty inherent to the scientific method that allows scientists’ vulnerabilities to magical thinking, scapegoatism, and moral panics to enter their work and color their results.
3. Conclusion
Sugar occupies a unique role of being regarded as both a food and a drug. It is this dual role that allows it to play the part of both nutritional scapegoat and demonized intoxicant. Attitudes and beliefs about foods and drugs express deep tensions between pleasure and asceticism, intoxication and restraint. Indeed the famous “marshmallow studies” in psychology have been held up to show how failure in impulse control (with sugar) is indicative of life long characterological weakness (Mischell, Ebbesen, and Raskoff Zeiss). By contrast, restraint from gobbling up marshmallows promises sobriety, willpower, moral superiority, and slenderness. Increasingly such marshmallow-resisting traits are even characterized as good “executive functioning”—a neurological concept that suggests, in the parlance of Western culture, that if one impulsively eats the marshmallow as a child, one is biologically destined for failure (consistent with the chemical imbalance theory that reigns king).
There are many reasons to regulate Big Food, decrease global sugar consumption, and fight back against hyperpalatable foods. It may be one of the only effective ways to fight against the powerful and corrupt sugar lobby in protecting public health. It could stem the tide of overweight, obesity, and sugar-related disease. It could protect those in poverty who are disproportionately marketed to by the sugar and soda industries. These potential outcomes make it an important matter of social justice.
Obesity and addiction researchers Kelly Brownell and Mark Gold reveal how a public health agenda drives the research when they say, “If certain foods or their constituents could be considered addictive, there might be justification for restricting their marketing, particularly to vulnerable populations such as youth” (xii). But ultimately this should be an empirical question. Calling something addictive that’s not, or broadening the addiction construct as a means of accomplishing social justice, is semantic and political, not scientific. While perhaps the science may eventually prove that sugar is a dangerous addictive substance, conclusive evidence for that is currently lacking. In the meantime, I suggest that by demonizing sugar as a public health menace we may be creating guilt and nutritional confusion where it is not necessary. Rather than throw the baby out with the bathwater, perhaps we would do well to remember that the dose makes the poison.
Works Cited
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington: American Psychiatric P, 2013. Print.
Avena, Nicole M., Pedro Rada, and Bartley G. Hoebel. “Evidence for Sugar Addiction: Behavioral and Neurochemical Effects of Intermittent, Excessive Sugar Intake.” Neuroscience & Biobehavoral Reviews 32.1 (2008): 20-39. Print.
Bartoshuk, Linda M. “Sweetness—History, Preference, and Genetic Variability.” Food Technology 45.11 (1991): 108-13. Print.
Becker, Howard S. “Becoming a Marihuana User.” American Journal of Sociology 59.3 (1953): 235-42. Print.
Blum, Kenneth, et al. “Neuro-Genetics of Reward Deficiency Syndrome (Rds) as the Root Cause of ‘Addiction Transfer’: A New Phenomenon Common after Bariatric Surgery.” Journal of Genetic Syndromes & Gene Therapy S.2 (2011): n. pag. Web. 9 Mar. 2016.
Blundell, John, Sarah Coe, and Beth Hooper. “Food Addiction—What Is the Evidence?” Nutrition Bulletin 39.2 (2014): 218-22. Print.
Brownell, Kelly D., and Mark Gold. Food and Addiction: A Comprehensive Handbook. Oxford: Oxford UP, 2012. Print.
Cargill, Kima. “The Myth of the Green Fairy: Distilling the Scientific Truth About Absinthe.” Food, Culture and Society: An International Journal of Multidisciplinary Research 11.1 (2008): 87-99. Print.
---. The Psychology of Overeating: Food and the Culture of Consumerism. London: Bloomsbury Academic, 2015. Print.
Castillo, Richard. Meanings of Madness. Pacific Grove: Brooks/Cole, 1997. Print.
Corsica, Joyce A., and Bonnie J. Spring. “Carbohydrate Craving: A Double-Blind, Placebo-Controlled Test of the Self-Medication Hypothesis.” Eating Behaviors 9.4 (2008): 447-54. Print.
de la Monte, Susanne M., et al. “Dysfunctional Pro-Ceramide, ER Stress, and Insulin/IGF Signaling Networks with Progression of Alzheimer's Disease.” Journal of Alzheimer’s Disease 30 Supplement 2.0 (2012): S217-29. Print.
de la Monte, Susanne M., and Jack R. Wands. “Review of Insulin and Insulin-Like Growth Factor Expression, Signaling, and Malfunction in the Central Nervous System: Relevance to Alzheimer's Disease.” Journal of Alzheimer’s Disease 7.1 (2005): 45-61. Print.
Derrida, Jacques. Points...: Interviews, 1974-1994. Stanford, CA: Stanford UP, 1995. Print.
Drewnowski, Adam, et al. “Sweetness and Food Preference.” The Journal of Nutrition 142.6 (2012): 1142S-48S. Print.
Freud, Sigmund. The Complete Introductory Lectures on Psychoanalysis. New York: WW Norton, 1966. Print.
Gearhardt, Ashley, et al. “Can Food Be Addictive? Public Health and Policy Implications.” Addiction 106.7 (2011): 1208-12. Print.
Gearhardt, Ashley, Michael Roberts, and Marice Ashe. “If Sugar Is Addictive What Does It Mean for the Law?” The Journal of Law, Medicine & Ethics 41 (2013): 46-49. Print.
Gearhardt, Ashley, William Corbin, and Kelly Brownell. “Preliminary Validation of the Yale Food Addiction Scale.” Appetite 52.2 (2009): 430-36. Print.
Gold, Mark S., William S. Jacobs, and Kimberly Frost-Pineda. “Overeating, Binge Eating, and Eating Disorders as Addictions.” Psychiatric Annals 33.2 (2003): 117-22. Print.
Goode, Erich., and Nachman Ben-Yehuda. Moral Panics: The Social Construction of Deviance. London: Wiley, 2010.
Gray, Gregory E. “Diet, Crime and Delinquency: A Critique.” Nutrition Reviews 44. Supplement 3 (1986): 89-94. Print.
Grob, Charles S., et al. “Pilot Study of Psilocybin Treatment for Anxiety in Patients with Advanced-Stage Cancer.” Archives of General Psychiatry 68.1 (2011): 71-78. Print.
Hanna, Joel M., and Conrad A. Hornick. “Use of Coca Leaf in Southern Peru: Adaptation or Addiction.” Bulletin on Narcotics 1.006 (1977): 63-74. Print.
Hebebrand, Johannes, et al. “‘Eating Addiction’, Rather Than ‘Food Addiction’, Better Captures Addictive-Like Eating Behavior.” Neuroscience & Biobehavioral Reviews 47 (2014): 295-306. Print.
Ifland, Joan R., et al. “Refined Food Addiction: A Classic Substance Use Disorder.” Medical Hypotheses 72.5 (2009): 518-26. Print.
Levinovitz, Alan. The Gluten Lie: And Other Myths About What You Eat. New York: Regan Arts, 2015. Print.
Lustig, Robert H., Laura A. Schmidt, and Claire D. Brindis. “Public Health: The Toxic Truth About Sugar.” Nature 482.7383 (2012): 27-29. Print.
Malik, Vasanti S., et al. “Sugar-Sweetened Beverages, Obesity, Type 2 Diabetes Mellitus, and Cardiovascular Disease Risk.” Circulation 121.11 (2010): 1356-64. Print.
Malik, Vasanti. S., et al. “Sugar-Sweetened Beverages and Risk of Metabolic Syndrome and Type 2 Diabetes: A Meta-Analysis.” Diabetes Care 33.11 (2010): 2477-83. Print.
Malik, Vasanti. S., Matthias B. Schulze, and Frank. B. Hu. “Intake of Sugar-Sweetened Beverages and Weight Gain: A Systematic Review.” The American Journal of Clinical Nutrition 84.2 (2006): 274-88. Print.
Malik, Vasanti S., and Frank B. Hu. “Sweeteners and Risk of Obesity and Type 2 Diabetes: The Role of Sugar-Sweetened Beverages.” Current Diabetes Reports 12.2 (2012): 195-203. Print.
Mennella, Julie A., and Gary K. Beauchamp. “The Early Development of Human Flavor Preferences.” Why We Eat What We Eat: The Psychology of Eating. Ed. Elizabeth D. Capaldi. Washington, DC: American Psychological Association, 1996. 83-112. Print.
---. “Early Flavor Experiences: Research Update.” Nutrition Reviews 56.7 (1998): 205-11. Print.
Mischel, Walter, Ebbe B. Ebbesen, and Antonette Raskoff Zeiss. “Cognitive and attentional mechanisms in delay of gratification.” Journal of Personality and Social Psychology 21.2 (1972): 204–218. Print.
Natella, Stefano, et al. Sugar Consumption at a Crossroads. Credit Suisse Research Institute, 2013. Web. 9 Mar. 2016. <https://publications.credit-suisse.com/tasks/rende...>
Preskorn, Sheldon H. “Ketamine: The Hopes and the Hurdles.” Biological Psychiatry 72.7 (2012): 522-3. Print.
Satel, Sally, and Scott O. Lilienfeld. Brainwashed: The Seductive Appeal of Mindless Neuroscience. New York: Basic Books, 2013. Print.
Schatzker, Mark. The Dorito Effect: The Surprising New Truth About Food and Flavor. New York: Simon & Schuster, 2015. Print.
Shroder, Tom. Acid Test: LSD, Ecstasy, and the Power to Heal. New York: Penguin, 2014. Print.
Slater, Lauren. “How Psychedelic Drugs Can Help Patients Face Death.” New York Times. New York Times. 20 Apr. 2012. Web. 9 Mar. 2016.
Smith, Julia Llewellyn. “John Yudkin: The Man Who Tried to Warn Us About Sugar.” Economic Policy Journal (2014). Web. 6 Mar. 2016.
Taubes, Gary. “What If It’s All Been a Big Fat Lie?” The New York Times Magazine. The New York Times. 7 July 2002. Print.
Vanderschuren, Louk, and Barry J. Everitt. “Drug Seeking Becomes Compulsive after Prolonged Cocaine Self-Administration.” Science 305.5686 (2004): 1017-19. Print.
Verebey, Karl, and Mark S. Gold. “From Coca Leaves to Crack: The Effects of Dose and Routes of Administration in Abuse Liability.” Psychiatric Annals 18.9 (1988) 5:13-20. Print.
Volkan, Vamik D. “The Need to Have Enemies and Allies: A Developmental Approach.” Political Psychology (1985): 219-47. Print.
Volkow, Nora D., et al. “The Addictive Dimensionality of Obesity.” Biological Psychiatry 73.9 (2013): 811-8. Print.
Willy Wonka & the Chocolate Factory. Dir. Mel Stuart. Warner Home Video, 1971. DVD.
World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective. Washington DC: AICR: American Institute for Cancer Research, 2007. Print.
Ziauddeen, Hisham and Paul C. Fletcher. “Is Food Addiction a Valid and Useful Concept?” Obesity Reviews 14.1 (2013): 19-28. Print.
Ziauddeen, Hisham, Sadaf Farooqi, and Paul C. Fletcher. “Obesity and the Brain: How Convincing Is the Addiction Model?” Nature Reviews Neuroscience 13.4 (2012): 279-86. Print.
Figures
Fig. 1: Jennifer. Free Candy Van. LivingInMyCar. 18 Nov. 2009. Web. 15 Dec. 2016. JPEG. <http://livinginmycar.com/blog/2009/11/19/unnamed-person-is-not-happy-about-this-blog/free-candy-van-2>
Fig. 2: Monod, F. L'Absinthe, c'est la mort!, 1905. Musée Virtuel de l’Absinthe. n.d. Web. 15 Dec. 2015. JPEG. <http://www.museeabsinthe.com/absintheAFFICHES4.htm...>
Fig. 3: Audino. Vote de la Chambre des Députés, 12 Février 1915. Musée Virtuel de l’Absinthe. n.d. Web. 15 Dec. 2015. JPEG. <http://www.absintheoriginals.com/posters.html>
Fig. 4: Conférénce Apache, postcard. ca. late 19th century. Musée Virtuel de l’Absinthe. n.d. Web. 15 Dec. 2015.<http://www.museeabsinthe.com/absintheCARTES4.html>
Fig. 5: Reefer Madness (Tell Your Children), 1936. Movie Poster. n.d. Web. 15 Dec. 2016. JPEG. <http://www.imdb.com/title/tt0028346/?ref_=ttqt_qt_...>